

If you’ve ever wondered what all those leads and sticky dots were doing when placed over a patient in a hospital or in a film then they were probably having their heart monitored. And by monitored, they were probably having some form of ECG (Electrocardiogram . . . with a C, for Cardio. Not EKG, like how the septics spell. ECG!).
ECG’s are a fantastic system used in lots of hospital and pre-hospital environments to help determine cardiological issues and help us determine the correct course of treatment and outcome for the patient.
They measure the electrical output of the heart and we do this by strategically placing several (10 in the UK) sticky dots attached to leads, over the patient’s chest and limbs. And, after the patient remains still, we gain a readout from the Lifepak machine that gives us 12 different views of the heart. This is when we, the clinicians, pretend to know what we’re looking at.
So below, to help anyone who might be in the remote bit interested, I’ve put together a quick Top 10 Do’s and Don’ts of how to ECG . . .
 1)
1)
Do . . .
-Gain consent from the patient.
This is quite an intrusive and personal procedure that will probably require elements of exposure. You will need to explain your procedure and what it entails so that they have ‘informed consent’ to say yes or no. The same applies with paeds – making sure parents are on hand for the procedure.
-Also, if there is gender difference, you will need to gain extra consent that this is ok – possibly giving the patient an opportunity for a female to perform the procedure of for one to act as ‘chaperone’.
Do not . . .
-Just whip up the patient’s top and start playing with their bra.
-Start slapping ECG dots over the patient’s body and moving body parts as if they are a rag doll.
Such simple disregard will probably result in a) slap, punch, kick, bite, spit, headlock, choking, and b) suspension, disciplinary, law suit, and possible striking off the register.
2)
Do . . .
-Tell the patient what you are doing and keep them informed as you go along. It’s all very well to get consent to do the procedure but every time you go to expose or touch the patient in private areas, then they need to be informed and consensual. This means almost every move has to be told to the patient. This also makes everything heard by those around and will come across a lot more professional than if you don’t.
Do not . . .
-Suddenly lunge at the patient and start ripping at the leads and dots to get them off.
-Make a grab at their breasts and start moving them around whilst having a nonchalant conversation about break times with your crew mate.
-Start shaving the hairs off the patient’s chest whilst whistling inane tunes
-Keep the parents of paeds outside and telling them, “we’ll be done in a minute luv”
All of these and any similars are generally deemed as assault and will see you sacked and in court.
3)
Do . . .
-Keep the patient’s dignity as best you can ie keep them covered whenever you can
Remember, this is a personal examination and all efforts in affording the patient their dignity should given.
-Try making sure you have female performing the procedure on a female and vis versa. -Leave the room or truck if you are gender opposite and someone else is doing the procedure.
-You can ask the patient or their friend to undo their own bra and lift it above their breasts whilst keeping the top down – look away whilst this is being done.
-If they’re wearing a blouse etc you could explain what you’re about to do and only lift the top when placing the dots – then place the top back down to keep them covered.
-If you have to “strip” the patient to expose the area then explain confidently, gain consent, and do so quick and simply – then have something (blanket or gown) to cover the patient immediately with.
Do not . . .
-Pull the patient’s clothes off down to their socks, throw them out into the street, then stand back and gawp.
-Ask everyone to leave, including partner, family and crew mate – slip on some easy listening music, dim the lights and start taking off your clothes as well as the patient’s
-Leave the patient exposed with breasts or shaven chest on show, for everyone to see. This includes when the back door is being opened on arrival to hospital, or when the patient is being carted in to the hospital on the trolley bed
All of these are frankly weird and wrong. Arrest, prison, sacking and beatings will probably follow.
4)
Do . . .
-Be professional in your approach, from start to finish.
-Be kind and impartial to the patient’s appearance and presentation
-Offer no judgements and treat all patient’s the same
Lots of the patients you perform ECG’s on will have weird and wonderful body shapes and ailments. Some will have super huge breasts, some won’t have any. Some will have false breasts, some will have strange shaped ones. Some will be grizzly bear hairy, some will have metal work all over. Some will smell insane, some will have sores and the like. Your job is to keep it professional and show nothing in your expression, movements and actions, and afford each and every patient the decency they deserve.
Do not . . .
-Expose the patient’s breasts, stand back, fold your arms, and say approvingly, “Oh wow”.
-Juggle the patient’s breasts in your hands whilst making “WEY-HEY” noises
-Tune in to Tokyo!
-Place a pith helmet on your head, grab a machete and shout, “I’m going in!”
-Say, “Oh my god I think I’m going to be sick” then promptly vomit violently over the patient and the ambulance floor
-Say, “We could make at least a kilo with that amount of breast cheese”
-Dress up in every piece of CBRN kit available, lean in to the patient and through a gas mask say, “Don’t worry luv, I’ve tied my ankle to the bench post”
Any of these or similar will – unsurprisingly – see you sacked, beaten, arrested etc . . .
5)
Do . . .
-Prepare the area to have the dots appropriately. This will mean possibly using clinel wipes or tissue to clean and dry the area. It may mean the use of a razor to shave the specific areas.
-Only clean or shave the intended areas.
If you are placing the leads on a ‘real’ heart attack patient, chances are they will be sweating – a lot! You will need to dry the areas in question quickly and then place the dots.
If they are dirty or there is inevitable “breast cheese” then this too, will have to be cleaned away, as long as it is covering the area intended for the leads.
If the patient is excessively hairy then only shave the areas needed for the dots.
Do not . . .
-Scrape up the “breast cheese” in one hand and fling it on the floor or smear it over the wall.
-Shave a penis shape, a random person’s name, smiley face into the patient’s chest hair
-Do not use imac cream or be tempted to burn the hair off.
6)
Do . . .
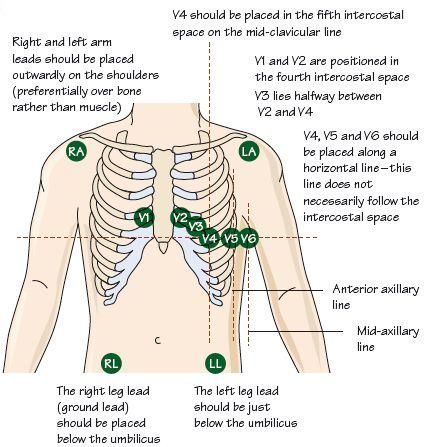
-Place leads correctly!
-Take your time in counting down the intercostal spaces for V1 and V2. A simple rule of thumb is that the 4th intercostal space is subtly above the nipple line . . . this is in people with ‘normal’ nipple lines.
-Make sure there is the subtle “pattern” to the placements.
-Place the chest leads on top of excessively large breasts instead of underneath. This will be the choice of the clinician but look at this way – if the breasts are huge and you place the dots underneath, then almost guaranteed V3 to V6 will be way out of place. This can and probably will have a slight effect on the outcome of the reading. By placing them on top of the breasts the electrical reading will still travel through the tissue in a line. And this will produce a ‘truer’ reading.
-Place the limb leads either on the extremities or at the proximal points (as in the picture). Either is acceptable. You may find the latter more useful in patients with ‘the shakes’
-Check that all the leads are the right way round and have remained stuck to the patient
Do not . . .
-Place V1 and V2 at 2nd intercostal spaces unless there is specific reason to do so. It’s the wrong place
-Have the leads the wrong way wound or in wrong order – and then start panicking at your printout!
-Incorporate a fork lift truck to hoist the patient’s breast back and then place V3, 4, 5 and 6 underneath. They will probably take readings on the patient’s lower intestines.
-Start placing defib pads “just in case” . . . unless they are definitely “about to go”
7)
Do . . .
-Perform an ECG for appropriate reasons.
ECGs are part of your tool kit for diagnosing and/or ruling out. There are clear times when it is not needed – for example, a simple trip up a step with no injuries or complaints. Most times, your reasoning for doing an ECG should come from the patient’s history and presentation.
Saying this, there should be nothing wrong with getting a 4 lead on sooner rather than later in cases of chest pains with suspected cardiac origin.
-Do subsequent ECGs in cases of any suspected cardiac chest pains.
Your first ECG might actually look fine . . . but if they’re having an MI, you watch that ECG change!
-Learn to read an ECG and learn the basics
-Treat the patient, not the machine!
This is hopefully something that is drummed in at school.
Finding simple AF in a patient with no presentation and relevant history is not a cause for panic.
Do not . . .
-(as above)Do an ECG if it’s not necessary eg “Ouch, I’ve just fallen off my bike and hurt my ankle” – “Right, Get your kit off, I want to do an ECG”.
-Just do the one ECG in the case of acute chest pain, and consider it ‘Normal Sinus Rhythm’ and leave the patient at home . . . and wonder why you keep getting Coroner’s statements.
-Stare horrifically at the ECG as if the world is going to explode – and completely ignore your patient in front of you.
-Shock the patient – ‘cos you saw what looked like VF on the screen’ even though you were laughing and joking with the patient at the time. This was probably ‘interference’.
-Chop the patient’s head off because the printout showed asystole whilst they were talking to you. The patient is NOT a zombie and you probably had some misplaced leads.
-Hold the ECG upside down but still pretend you know what you’re looking at
8)
Do . . .
-Explain your findings to the patient
This includes explaining that you think they may be having a heart attack, should the ECG show this along with the history and presentation. Be bold, confident and professional – the patient will be looking to you for ANY support they can get at this stage.
-Explain your plan of action
The patient, in worse case scenarios, will be thinking the worse. This is your time to come through and show the glimmer of hope they are looking for. Be kind caring and positive. Give them a plan of action they feel confident and happy with, and follow it through.
-Treat the patient appropriately and take them to the appropriate place for ongoing treatment.
If they’re in pain, treat it. If they’re having a heart attack, take them to a heart attack centre.
Do not . . .
-Suddenly see the blatant MI on the printout, look panicked, turn away from the patient biting your fist and say, “Everything’s fine”
-Panic and run out of the ambulance screaming. Likewise, don’t flounder, cry or sob and then start throwing any medicines you can find at the patient.
-Leave a blatant MI at home with a GP referral
-Take a perfectly normal pain free NSR patient to a cath lab
-Decide you can’t be arsed to give this MI patient morphine, cos you think they’re a dick
9)
Do . . .
-Remove dots from patients that aren’t conveying. Prerogative over removal if conveying.
-Help clean the patient and redress them if needs be
Do not . . .
-Leave dots in place so that the patient forgets about them – especially the ones under the armpit! – and they start festering and causing infections at a later date.
-Throw the patient’s clothes at them and shout, “We’re done! Seeya!”
10)
Do . . .
-Mark your findings and subsequent findings on your paperwork
-State why you have or haven’t done an ECG on your paperwork. If you’re not doing so, be confident in stating why on your PRF.
Do not . . .
-State on your PRF, “All obs fine – pt left at home” when they’re having a raging MI
-Leave a ‘chest pain’ patient at home with no explanation on your PRF of why you have or haven’t done an ECG.
-State on your PRF, “They were dead when I found them”
ECG’s are wonderfully useful tools of the trade. They certainly help diagnose problems and help rule out others. If you can, and haven’t done so already, get yourselves on extra courses to learn them. There are also plenty of books and online systems out there to help in understanding, as well as good apps and YouTube videos.
Hope this has helped.
Binder
NB and please, really DO NOT shock a fake reading of VF.
Hi Binder
I assume all the “Do Not’s” have been learned through your own hard bitter
personal experience 😉
Never!!!
. . . . well, a bit. Maybe
OMG Breast cheese…. I HAVE never heard of that and it sounds absolutely horrific, luckily we don’t have that here in Canada. The bitterly cold weather, must keep us clean I guess. Hahaha
Thanks for the tips!! As an RN, additionally
I would add one thing: if a female patient would like to keep their bra on for the ECG for comfort, please let them., this is a FINE practice and will greatly ease the minds of the patient (As long as it doesn’t have a metal bone). In modern times, we are starting to recognize that a patients comfortability is of paramount concern… this could help attain less false negative results while maintaining the patients dignity.
Take good care and thanks a million
Gwendolyn
I agree. I do try and keep clothes and bits on a patient as much as possible – for dignity reasons. There are times I will ask the patient to “undo their bra, flip it up over their boobs, but keep their top down” and this is when the bra or other material causes interference in the nodes (ie rubbing of clothing to the nodes will cause un unclear image). But otherwise, bang on
This is absolutely fantastic!
Thank you for this!! I am a patient having my first ECG tomorrow. Had no clue what to expect, but the detailed explanation of this post has helped me tremendously. Informative and entertaining!! I think I love you now 😉
Thanks. I suspect if you’re having a routine ecg it will be very quick. Good luck. Ask for a copy of it if you can